Joint mobility of the hip plays a central role in the prevention of postural disorders, functional limitations, and age-related locomotor decline. According to World Health Organization data, over 35% of individuals aged 70 and over experience mobility limitations, with a rising prevalence of gait disorders and hip joint pain (WHO, 2015). Longitudinal cohort studies have shown that reduced hip mobility is associated with increased risk of dependence, falls, and diminished quality of life (Verghese et al., 2006; Muir et al., 2010). These findings underscore the urgency of targeted preventive and therapeutic strategies for this strategic joint. The hip, positioned between the trunk and lower limbs, contributes to pelvic stability and force transmission to the ground. Its mobility influences gait fluidity, stride efficiency, and the ability to produce explosive or precise movements in sport. However, it is highly vulnerable to stiffness, functional restriction, and progressive degradation due to orthopedic, neurological, post-traumatic, or sedentary causes. Epidemiological studies confirm that reduced hip range of motion is a major risk factor for loss of autonomy in older adults (Muir et al., 2010).
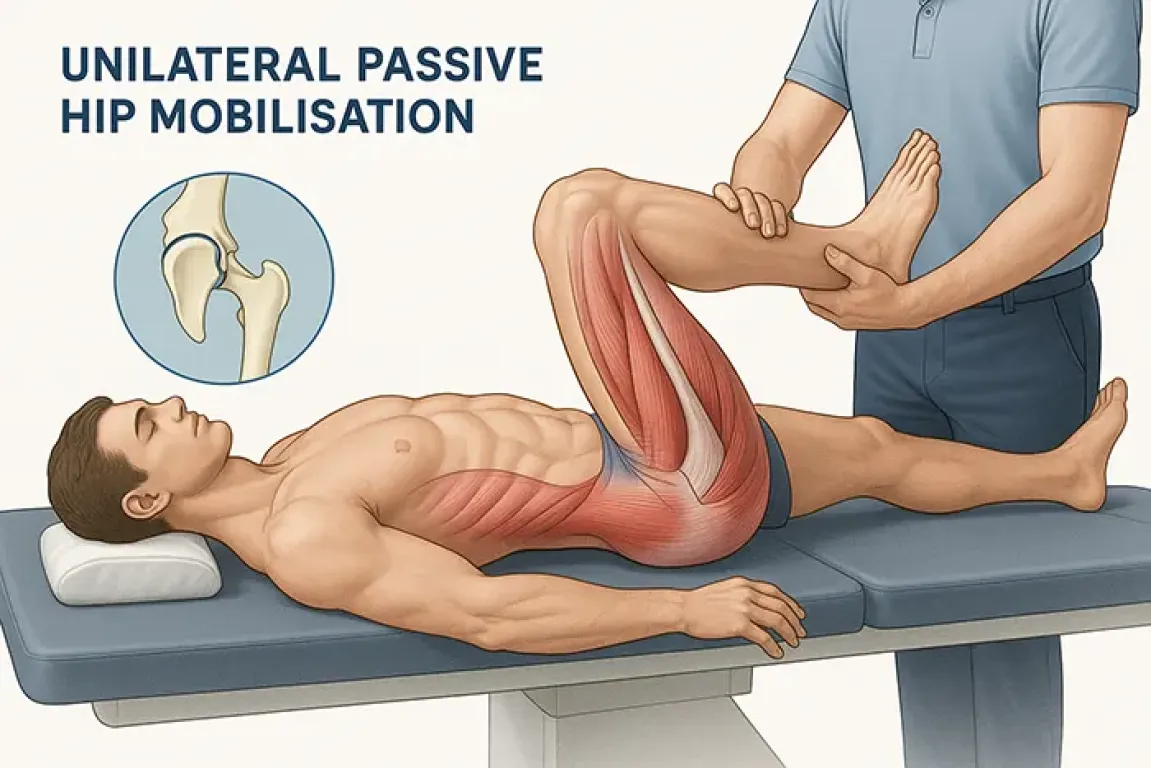
Unilateral passive mobilization of the hip, as offered by DPA Med® and DPA Sport®, introduces an innovative approach to mobility optimization without load constraint. By targeting one lower limb at a time, it allows for gentle yet deep tensioning of capsuloligamentous structures while triggering reflex neuromuscular reorganization that supports functional plasticity. This decompression-based movement, coupled with a complex trajectory that replicates natural gait patterns (particularly lemniscate motion), proves highly relevant for reactivating posterior and lateral muscle chains often underutilized in gait disorders or chronic functional deficits.
The lemniscate trajectory used by DPA Med® mimics the physiological swaying of the hip during walking. This figure-eight motion stimulates deep myofascial chains in three dimensions while activating proprioceptive receptors involved in muscle tone regulation. Research such as that by Huang et al. (2021) demonstrates that complex motor patterns inspired by natural gait promote stronger activation of sensorimotor cortical areas.
When applied without gravitational load, this rhythmic and spiral movement facilitates the progressive relaxation of contracted connective and muscular tissues, especially in spastic, orthopedic, or post-surgical conditions. It also triggers archaic postural reflexes through activation of polysynaptic spinal circuits, critical for functional recovery in neurologically impaired patients.
Integrating this technique into comprehensive rehabilitation aligns with literature on multisensory stimulation (Shumway-Cook & Woollacott, 2012) and the effects of three-dimensional mobilization on cortical plasticity (Liepert et al., 2000). In this sense, DPA Med® functions not only as a mechanical device but also as a neurofunctional stimulator, fostering coherence between reflex muscle activation, tonic release, and postural integration.
The slow, rhythmic stimulation induces progressive myofascial release, which is not merely mechanical but also neuromodulatory. It influences muscle tone via proprioceptive receptors such as muscle spindles and Golgi tendon organs (Chaudhuri et al., 2022). By reducing excitability in gamma motor neuron circuits, this technique lowers baseline tone—crucial in chronic spastic or painful conditions and beneficial for enhancing functional readiness in sport. The stimulation frequency used is near-optimal for achieving durable neuromuscular relaxation, as suggested by studies on manual therapy and mechanical vibration (Laufer et al., 2001).
This tonic modulation also reactivates archaic reflexes by reducing central inhibition and unlocking subcortical motor circuits, aided by the sensory-controlled supine environment. Neurophysiological research indicates that archaic reflexes can be inhibited by gravitational and cortical constraints but reemerge under neuromuscular relaxation. Literature in neurological rehabilitation, including Bobath-based approaches and sensorimotor integration studies, confirms that targeted proprioceptive stimulation can reengage primitive motor patterns essential for restoring integrated motor control. In the absence of gravity, the CNS is primed to rediscover foundational motor schemes. Once reintegrated, these reflexes enable smoother transition to upright motion, serving as a foundation for postural and locomotor reprogramming. Benefits are seen across all gait phases—step initiation, propulsion, and landing—via reactivation of subcortical sensory-motor loops often compromised in chronic neurological conditions (Dietz et al., 2002).
.webp)
This approach targets a broad spectrum of conditions: early or post-operative hip disease, hip osteoarthritis, femoroacetabular impingement, post-hip replacement rehabilitation, post-stroke mobility limitation, hemibody spasticity, pelvic fracture recovery, muscle injuries (psoas, gluteus, piriformis), post-surgical sciatica, iliotibial band syndrome, and unilateral compensation due to weight-bearing or functional asymmetry. It also includes central and peripheral gait disorders, such as hemiparesis, Parkinson’s syndromes, and proprioceptive neuropathies. In all cases, reduced pathological tone creates a more effective therapeutic window for motor reprogramming.
In sports, this technique is valuable for athletes relying on lower limbs: sprinters, jumpers, footballers, rugby players, dancers, triathletes. Unilateral passive mobilization promotes deep myofascial release, improves hip-trunk dissociation, and optimizes pre-activation capacity during weight transfer. Schleip et al. (2012) emphasize the fascia’s sensory role in tone modulation. For amateur athletes, this technique offsets asymmetry-induced imbalances. For professionals, it primes neuromuscular systems for better segmental coordination, reducing injury risk and enhancing high-intensity mechanical readiness. Combining myofascial release with reflex activation of deep muscles—e.g., involuntary recruitment of transversus abdominis and multifidi, confirmed by ultrasound—improves dynamic muscle engagement. Tone regulation also enhances explosive contractions in push-off, impulse, or directional shifts. These effects align with Behm & Chaouachi (2011) on neuromuscular preparation in injury prevention and performance.
Physiologically, the technique’s efficacy arises from several mechanisms. In the absence of gravity, joint unloading promotes relaxation of deep muscle chains, facilitating axial joint movement. This relaxation lifts spinal reflex inhibition and facilitates future motor group activation. Passive work also enables gradual myofascial stretching, modulating spindles and reducing pathological co-contractions. Moreover, slow segmental discharge movement generates proprioceptive input processed preferentially at spinal and supraspinal levels, strengthening motor integration pathways. The lemniscate motion produces alternate hip lateralization, stimulating commissural and corticospinal circuits critical to gait (Courtine et al., 2006).
The observed carryover effect—lasting functional improvement post-stimulation—is explained by neuromotor reprogramming. Even without conscious awareness, users integrate new motor patterns reflexively. This motor plasticity relies on well-documented neurophysiological processes, including long-term potentiation (LTP) in sensorimotor circuits, strengthening cortico-spinal loop synapses, and facilitating corticospinal and reticulospinal transmission (Kleim & Jones, 2008; Nudo, 2013). The resulting automation yields smoother movement, greater pelvic stability, and reduced strain on compensatory chains. This motor memory becomes more lasting with repeated sessions, which structurally consolidate neural networks governing postural and locomotor control.
This mobilization also supports functional longevity. By maintaining joint amplitude, regulated tone, and effective inter-muscular coordination, it slows locomotor decline with aging. Studies confirm that hip mobility loss predicts dependency, falls, and reduced healthy life expectancy. Restoring fluid, pain-free motion prevents age-related musculoskeletal disorders and enables sustained physical activity—a key health asset. The anti-gravity effect of passive mobilization, by eliminating joint loading, makes it suitable even for frail or painful individuals, enhancing its role in healthy aging (Studenski et al., 2011).
DPA Med® and DPA Sport® are thus unique tools for pain-free, fatigue-free activation of the deepest components of human movement. Used regularly—two to three times per week for 10 to 20 minutes per session—they enable sustainable rehabilitation, targeted prevention, and optimized performance, while honoring the foundational principles of neuroplasticity, joint physiology, and reflex tone regulation.
Author: Christophe BENSOUSSAN with the help of AI - Image credits ©ChatGPT